
In one year, I reversed early-stage osteoporosis without bisphosphonates. Using a combination of hormone replacement therapy (HRT), high-force mechanical loading, and a whole-food plant-based diet with targeted supplementation, I increased bone density by 6.8% at the lumbar spine and 7.2% at the femoral neck while traveling more than half the year.
Last week (in June 2026), in my endocrinologist’s office, I watched his expressions as he stared at his computer monitor. His eyes narrowed, and he mumbled some numbers, again, and then again. He looked straight at me for a moment with narrowing eyebrows and said, “Did you take the Fosamax?” I said, “No”, with a smile that I tried hard to suppress.
The doc was looking at my DEXA scan numbers, which I had already seen, internalized, and researched ahead of the appointment. He was seeing it for the first time, and he looked utterly puzzled. By the end of the appointment, he was beaming with joy, congratulating me, and reducing my appointment frequency to every 6 months. I was estatic.
Background and My Belief System
I was first sent to my endocrinologist in August 2024 at the onset of Graves’ disease. Hyperthyroidism, coupled with menopause, had taken a toll on my bones. By April 2025, the numbers were clear. My bones were full-on in osteoporosis. At my 2025 appointment, I pleaded with him to give me just one year to try to tackle the osteoporosis without bisphosphonate drugs.
My approach is to resolve root causes rather than simply manage symptoms, with a bias on lifestyle first. I work with specialists, do my own research, and decide on a case-by-case basis where lifestyle change is enough and where I need medical support. As an example, for my bones, that meant avoiding bisphosphonates (and their side effects) but accepting HRT. In my case, HRT addresses the root cause by replacing the estrogen my body had stopped producing. It’s a nuanced distinction, not entirely black-and-white.
In this article, I’m sharing my personal journey, not medical advice. My goal is to share my experience in reversing osteoporosis with minimal medications, so you or someone you know may benefit from the approach or some of my learnings. Please work with your doctors and professionals before making any changes to your treatment plan.
The Full Picture of Osteoporosis: Four Years of Data
In this article, I will use customary medical terms. If you’re not familiar with them, I’ve added definitions further down.
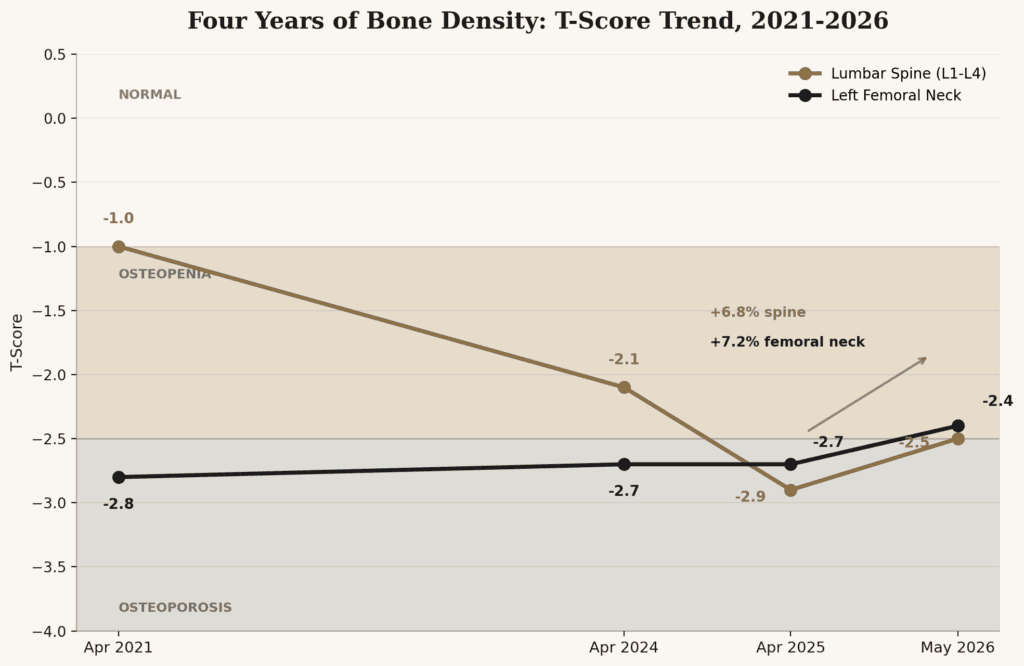
In April 2021, my lumbar spine T-score was -1.0. Borderline, but technically normal. My femoral neck score was already -2.8, which puts it in the osteoporosis range, though no one flagged it as urgent at the time. I was young, active, eating plant-based, working, and traveling constantly. I wasn’t particularly worried.
By April 2024, my lumbar spine score had dropped to -2.1.
By April 2025, it was at -2.9. In the span of four years, my spine went from the edge of normal to frank osteoporosis. The femoral neck held roughly steady through 2024, then dropped rapidly to -2.7 by April 2025.
A 9.4% ten-year probability of a major osteoporotic fracture.
See the exact DEXA numbers
Lumbar Spine (L1-L4)
| Date | BMD (g/cm2) | T-Score | Classification |
| Apr 2025 | 0.833 | -2.9 | Osteoporosis |
| May 2026 | 0.890 | -2.5 | Osteoporosis (+6.8%*) |
Left Femoral Neck
| Date | BMD (g/cm2) | T-Score | Classification |
| Apr 2025 | 0.657 | -2.7 | Osteoporosis |
| May 2026 | 0.704 | -2.4 | Osteopenia (+7.2%*) |
Statistically significant at 95% confidence level.
The spine numbers tell the clearest story. From 2021 to 2025, despite being active and eating well, my lumbar spine lost density every year. That four-year decline corresponds almost exactly to the perimenopause and menopause transition, with the sharpest drop in 2024-2025 when hyperthyroidism was added to the picture.
In 2026, the trajectory reversed.
What happened between 2021 and 2025 to cause the dip?
Short answer: Menopause and hyperthyroidism. Both conditions are known to accelerate bone loss. I had both at once.
The timing was not convenient. We had just returned from Japan. Nirmal had retired, and I was considering retiring at the end of the summer. Our goal is to visit every country and hike the prettiest places on the planet. We had already booked a 3-month round-the-world trip, which included Antarctica, Norway, Bhutan, and other countries. I’m used to climbing, hiking, and falling often. Plus, I hate pills.
The clinical advice was: be careful, take bisphosphonate-based osteoporosis medication, and do not fall.
I refused to accept any of this. So I looked for answers.
What Causes Osteoporosis with Menopause and Hyperthyroidism?
Both conditions accelerate bone remodeling. Bone is never static: the rate at which old bone is broken down normally matches the rate at which new bone is formed.
Cells called osteoclasts break down old bone, and cells called osteoblasts rebuild it. The remodeling cycle normally takes around 200 days. When osteoclasts work faster, the rebuilding side can’t keep pace, and you lose a small amount of bone density with each cycle.
Hyperthyroidism and Osteoporosis
Excess thyroid hormone, as in hyperthyroidism, directly speeds up that cycle. It pushes osteoclasts to become more active and more numerous, and it weakens the signals that would normally hold them back. Because resorption accelerates faster than formation can keep pace, each cycle ends in a small net loss. Over months, that adds up.
Faster bone turnover also dumps more calcium into the bloodstream than usual, and the body responds by excreting more of it and producing less of the hormone that helps you absorb calcium efficiently from food. That compounds the first problem.
Menopause and Osteoporosis
Estrogen keeps osteoclast activity in check. When estrogen drops during menopause, the check weakens. Most postmenopausal women without any intervention lose 1-2% of bone density per year.
So when hyperthyroidism and menopause overlap, you don’t get one problem on top of another. You get two separate signals pushing the same process in the same direction at the same time, which is part of why my decline between 2024 and 2025 was sharper than prior years.
Normalizing estrogen and thyroid function stops the acceleration, but it doesn’t reverse what’s already been lost. That part needed something actively working in the other direction.
One Year Later – In 2026
My endocrinologist was thrilled when my May 2026 DEXA scan showed increases in the lumbar spine and my left femoral neck. Both gains were statistically significant at the 95% confidence level. My radiologist’s impression used the word “significant” twice. I had both 2025 and 2026 readings on the same lab. These deltas were real, not noise.
A gain of nearly 7% at both sites, in one year, while traveling for over half of it, is not the expected outcome.
So what happened? I dived into research to unravel the mystery.
What Reversed Osteoporosis in My Bones?
There was no single intervention. It was three things working together. I don’t think any one or two of them alone would have produced these results.
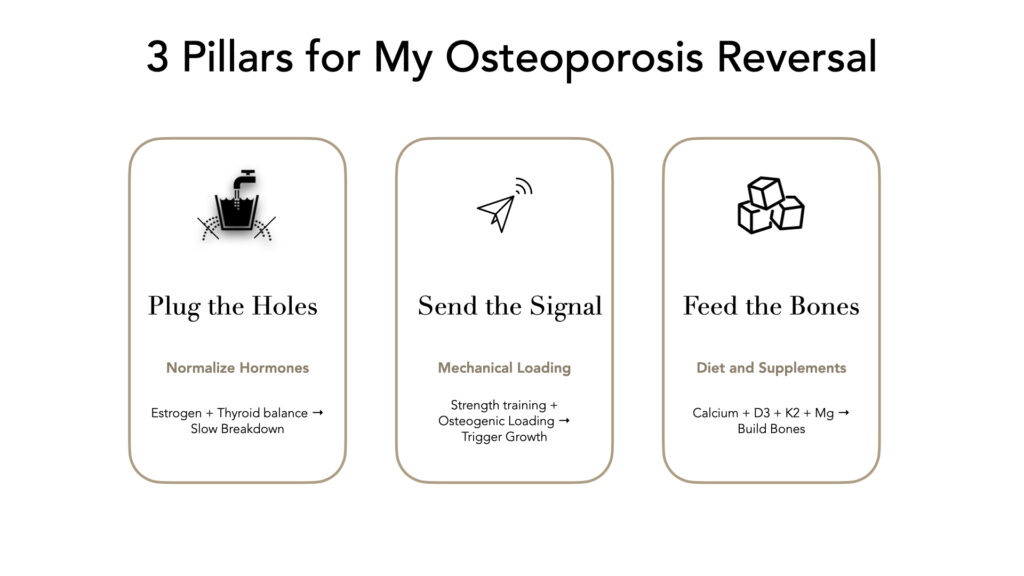
Plug the Holes: Estrogen and Thyroid
The analogy that made this clear to me: if you’re trying to fill a bucket, you have to plug any holes before you turn on the faucet. For postmenopausal women, declining estrogen creates a hole in the metaphorical bucket. Hyperthyroidism was the second one for me. Without addressing both, exercise and diet are fighting a losing battle.
I use bioidentical estradiol patches with progesterone to help build some estrogen. Plus, my hyperthyroidism was normalized by August 2025, which removed the second source of bone loss. So, I had two fewer things working against me.
Traveling with patches requires some organization. My doctor had recommended placing the patch on two set days each week, say Tuesday night and Saturday morning, so it becomes a habit. But that breaks down when we’re constantly changing time zones. So, I added two recurring weekly calendar events. The events adjust for time zone shifts automatically. There must be apps for this, too. I also engineered a sleep protocol for time zone changes that works well.
Secondly, it’s not easy to get estrogen patches when traveling to remote destinations, so I carry enough patches for long trips. That means when I’m home, I work with my pharmacist and doctor to get extras that’ll last until I’m back.
Send the Signal: Strength Training and Osteogenic Loading
Most osteoporosis advice eventually comes down to the same recommendation: lift weights. That’s right, but it undersells how specific bone actually is about what counts as a sufficient signal.
Strength Training
I work with a personal trainer for strength training when I’m not traveling. This matters for two independent reasons – (a) Muscle pulling on bone is itself a mechanical signal, gentler and more constant than a single intense session. And (b) most osteoporotic fractures happen because of a fall, not because of low bone density on its own. Stronger muscles and better balance lower the odds of falling, which is a form of protection in itself.
But I’m not lifting heavy enough weights in these sessions to effectively trigger bone growth and reverse the numbers. Bone doesn’t respond to gentle movement, or even the moderate resistance training most people can safely do with free weights. It responds to loads that exceeds its normal capacity by a wide margin, a different and much higher threshold than typical strength training reaches.


Osteogenic loading
That’s the job of a category of exercise called osteogenic loading: brief, very high force, well beyond what’s practical to load in the gym. OsteoStrong is the provider I use. The robotic equipment is calibrated to hit what the system calls the “rapid growth trigger”, a force threshold that will trigger bone growth.


Since May 2025, my upper-body pushing force has increased from 3.2x to 4.2x my body weight. My lower body went from 7.0x to a peak of 11.7x, currently at 10.5x. As the chart shows, I missed sessions when traveling.
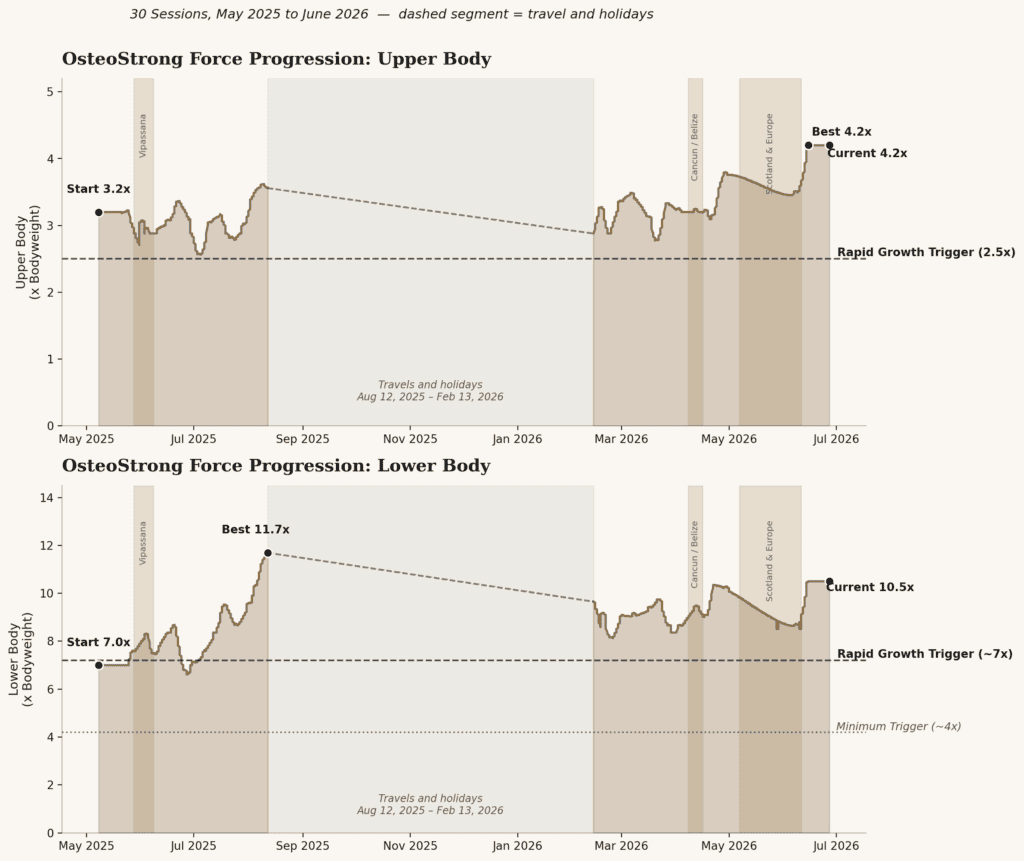
The difference between strength training and osteogenic loading is primarily a matter of dose. Osteogenic loading is a very high-force load held for about 10 seconds that directly triggers bone-building cells. Strength training consists of many smaller pulls, repeated over months, that indirectly reinforce the same bone through the muscle attached to it.
After my training session, I take a dose of creatine which helps my recovery time. The evidence for creatine improving muscle strength and lean mass in postmenopausal women, particularly when paired with resistance training, is fairly well established. The evidence for creatine affecting bone density directly is thinner and more preliminary. I take it for muscle strength, and treat any bone benefit as a possible bonus.
When Traveling
When I’m on the road, I can’t replicate either signal. What I can do: heel drops, anywhere, anytime. I’ve built a travel workout routine with my trainer and exercise physiologist, and I have to make it a habit. We hike up mountains when the destination allows it. For example, on the Tour du Mont Blanc trek, we carried a day pack and sometimes an overnight pack up to a few thousand feet.

On the recent five-week European trip, we started with 8-day hike in the Scottish Highlands and ended with a week of hikes in the spectacular Dolomites. It doesnt have the same impact as pushing 1,000 pounds for ten seconds, but it keeps the signal alive until I’m home. As a bonus, these mountains are so stunning and the experiences so wonderful, that they improve overall well-being on their own.
Feed the Bones: PBWF Diet with Targeted Supplements
I’ve written before about keeping a whole-food, plant-based diet on the road. This section is about what that diet needs to do specifically for bone health.
Calcium comes from greens, beans, tahini, natto, and many plant sources. I’m not meticulous about hitting an exact daily target, but I load up on plant-based whole foods.
The supplements I added are: calcium, vitamin D3, vitamin K2, and magnesium glycinate. If you’re new to K2, the short version is this: D3 increases calcium absorption, but K2 directs where that calcium actually goes. Without K2, absorbed calcium can deposit in arteries rather than bones. I take them together but space calcium at least an hour away from main meals so as to reduce interference with iron absorption from food.
Chronic inflammation is associated with accelerated bone loss. The anti-inflammatory effects of eating PBWF are probably a factor too, though they’re harder to quantify.

Glossary of terms
A few terms in this post come up often in osteoporosis care but aren’t everyday vocabulary. Here’s what they mean.
| Term | What it Means |
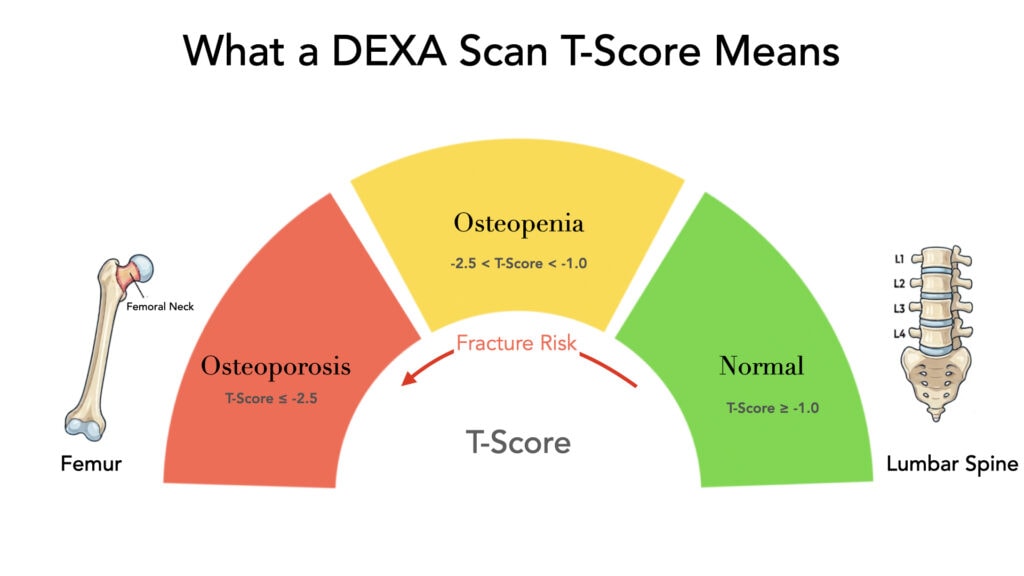
| DEXA (or DXA) scan | A low-radiation X-ray test that measures bone mineral density, usually at the spine and hip |
| BMD | Bone Mineral Density, the measurement a DEXA scan produces, expressed in g/cm² |
| T-score | Compares your bone density to that of a healthy 30-year-old of the same gender. WHO defines normal as -1.0 or above, osteopenia as -1.0 to -2.5, and osteoporosis as -2.5 or below |
| Z-score | Compares your bone density to people of your own age, gender, and body size, rather than to a healthy 30-year-old |
| Osteopenia | Lower than normal bone density that hasn’t yet reached osteoporosis levels |
| Osteoclast | A cell that breaks down old bone tissue. Bone loss happens when osteoclasts outpace bone-building cells |
| Osteoblast | A cell that builds new bone tissue |
| Bisphosphonates | A class of prescription drugs that slow bone breakdown, commonly prescribed as first-line for osteoporosis |
| Bioidentical estradiol | An estrogen formulation structurally identical to what the body produces. The term is used in both clinical and marketing contexts, so ask your doctor about the specific formulation rather than relying on the label |
| Graves’ disease | An autoimmune condition that causes the thyroid to become overactive (hyperthyroidism) |
| FRAX | A tool that estimates the ten-year probability of a major fracture, based on bone density and other risk factors |
What Traveling Half the Year Changes
The question I get from our community is some version of: “How do you keep a health routine going when you’re rarely home?” The honest answer is that you don’t maintain it perfectly. You maintain the most important parts and let the rest flex.
I don’t have an OsteoStrong in Madagascar, Bhutan, or anywhere else. But I do have the floor of any hotel room. And I carry resistance bands in my carry-on. In hotels or expedition ships, there’s usually a small gym. On hiking days, hiking is the training.
Many hotels have an elaborate healthy breakfast buffet with
- fresh veggie and fruit juices. In Italy, they have a juicing machine and chopped veggies to make your own juice
- spread of nuts, seeds, and nut milks
- protein-rich breakfast options without eggs and meats
- loads of veggies – fresh and cooked.

The choices are endless, and we make a point of touching base with the chef early. Trust me, they love to feed the guests well. A hearty brunch is our best source of macro- and micro-nutrients. We’re hitting the road fully nourished.
For destinations that don’t have elaborate breakfasts, I carry my supply of nuts, seeds, dried fruit, and some savory breakfast items to stay nourished. There is a trend of taking AG1-like products to get nutrients from veggies. I don’t like the taste, but I may adapt to it eventually.
What doesn’t flex: plant-based diet, supplements, and HRT. This trio travels in my bag to every country.
Where I Go From Here
One good year does not mean the problem is solved. The goal now is to continue the trajectory: maintain the gains and get annual follow-up DXA scans to confirm the trend is holding.
If you are navigating a similar diagnosis, I hope this is useful. Not as a protocol to copy, because what worked for me reflects my specific situation and my starting point. But as evidence that significant improvement is possible, and that traveling while taking this seriously is not a contradiction.
We live in a golden age when many experts and advanced and ancient protocols are accessible. But ultimately, we own our personal health journey. We owe it to ourselves to stay fit and serve. The buck stops with each one of us for our personal health.
If you found this useful, the longevity and travel section of this site has more on how we maintain a plant-based diet, stay active, and approach healthspan as a practice across 130+ countries.

Last Updated on July 30, 2026 by Jyoti Baid



sangeeta
July 10, 2026 @ 7:52 am
I just came across you blog yesterday, looking for Colorado tips. Oh, you inspire me ! I’m happy for you; you are healthy again and continue to travel . Best..
Kailash Kothari
July 11, 2026 @ 9:34 pm
That’s an amazing accomplishment and beautifully written blog, congratulations Jyoti! Great to see you travel the world while maintaining a plant based lifestyle and reversing your diagnosis.. amazing!